

01 Jul Donor-Supported Human Resources for Health Inventory Tool
What is the HRH Inventory Tool?
To better understand the scope and nature of donor-supported investments in the health workforce, the Human Resources for Health in 2030 (HRH2030) Program developed a tool to help countries inventory and analyze donors’ investments in health workers. The HRH Inventory Tool provides donors and host governments with a wealth of information about donor investments in the health workforce, from the job titles of health workers supported to the facilities where health workers are based, and includes detailed information on health workers’ gender, compensation, and professional development.
Why is an HRH Inventory needed?
PEPFAR, the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM), and other donors have invested millions of dollars to supplement the budgets of governments either to hire additional, contracted staff or to amplify the reach and effectiveness of existing staff through overtime pay, support for outreach activities, motivational benefits, and skills development. Donors and host governments need tools to better understand the scope and nature of staffing investments in order to optimize health worker utilization for advancing HIV epidemic control and inform sustainability planning for when epidemic control is achieved. Developing an inventory of HRH investments is the first step to understanding donors’ investments, and provides the data needed to answer critical questions, such as: who are the donor-supported workers, where they are located, what are their related functions and costs, and do they align with existing government structures and policies?
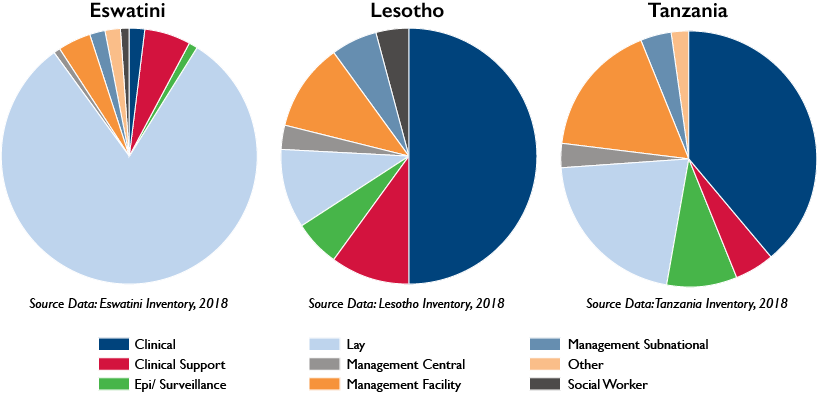
The HRH inventories in these three countries, above, have increased the understanding of the donor footprint in health workforce remuneration support in countries.
Where has the HRH Inventory been implemented?
The HRH Inventory has been deployed in 5 countries and tailored based on the country-context. HRH2030 developed the HRH Inventory in close collaboration with PEPFAR in Tanzania—a country that has been inventorying and analyzing its PEPFAR-supported health workforce since 2013. In 2018, the HRH Inventory was deployed in Tanzania to track PEPFAR-supported investments of more than 16,000 health workers. With support from PEPFAR in 2018-2019, HRH2030 expanded the application of the HRH Inventory to three additional countries—Lesotho, Eswatini, and Namibia—and included investments by other donors, most notably GFATM. In Lesotho, the HRH Inventory revealed how donors collectively are amplifying government staffing, and highlighted the need to rationalize lay cadres to support governments’ policies and task sharing models. In Eswatini, the HRH Inventory is influencing government-led HRH transition analysis and plans, and raised the visibility of facility-based, lay cadres. In Namibia, it is supporting PEPFAR programming and stakeholders consultations on how to sustain gains in HIV epidemic control, even as some donors plan for withdrawal. Most recently, with support from USAID, the HRH Inventory is being deployed in the Philippines to support the National Tuberculosis Program plan for the transition of GFATM supported-workers to local entities.
Who completes the tool and who is included?
Implementing Partners or Principal Recipients who provide direct financial support to health workers in the system should complete the HRH Inventory Tool. Ideally, the HRH Inventory Tool is completed prior to the end of the fiscal year to support end-of-year reporting and to inform subsequent year programming. It also can be a valuable exercise to refresh the data every six months, especially if there are significant shifts in workforce supports. In general, it is advised that the HRH Inventory only include support to health workers that support government’s HIV and TB epidemic control efforts, and therefore, reflects HRH investments that would need to be transitioned locally, if development partners were to immediately withdraw their support. Project staff that either coordinate or oversee donor activities or provide capacity building to the government or local partners should not be included. Hourly or temporary workers who are important to service delivery should be included in the Hourly Template, which is a streamlined version of the tool designed to focus on the hours, locations, and functions provided rather than the individual health worker.
How is it conducted?
First, the donor or host government should customize the HRH Inventory Tool for the country context. This involves determining the scope and timeframe for the Inventory, whether to add or delete any questions, and creating drop down boxes to streamline and produce consistent answers where possible, such as for the geographic locations and facility names. If the country reports through PEPFAR’s Data for Accountability, Transparency and Impact (DATIM), it is recommended to use DATIM’s categories and lists, such as cadre categories, facility names, etc., to allow additional analyses. Second, the donor or host government, should inform the Implementing Partners and Principal Recipients who provide direct support to health workers of the exercise and host a consultation to explain the HRH Inventory Tool and gather inputs on Tool refinement. A Point of Contact (POC) should be named by the donor or host government to respond to questions during the data entry phase and be the sole recipient of the data submitted. Once the data is submitted, the POC should review and validate the data with each implementer for completeness and consistency.
What happens next?
After the data for each implementer has been cleaned, it should be consolidated into an excel file. The data can now be analyzed using Pivot tables and dashboards to track and analyze investments in HRH staffing, down to the site level, for sector-wide performance monitoring and program planning. Other data points such as government pay scales, government staffing norms and monitoring, evaluation and reporting (MER) indicators can be incorporated into the data set for additional analyses. For example, if the government cadres and pay scales are available, the donor-supported workforce can be mapped to determine if the investments are well-aligned with public service. If there are priority hires, the HRH Inventory can be translated into a “back of the envelope” valuation of the potential costs to the partner country to absorb HRH investments, and models different transition scenarios and cost estimates as compared to country plans, priorities, and budgets.
How to access the tool:
To download a copy of the tool, visit the PEPFAR Solutions Platform.
Associated content:
Blog: Understanding the Donor-Supported Human Resources Needed to Achieve Sustained Epidemic Control
Country: Global
Resource Type: Tool
Topic: HIV/AIDS, Sustainability, HRIS and health workforce data, Performance and Productivity